Your Cart is Empty
How Low Testosterone Keeps Men Single


The average 25-year-old man today has the testosterone of a 40-year-old man in 1987. Nobody is talking about what it's doing to his relationships.
There is a number your doctor almost certainly hasn't mentioned. It's the percentage by which average testosterone has fallen in young American men over just 17 years: 25%[1]. Not in elderly men. Not in the sick or sedentary. In men aged 15 to 39.
At the same time, 63% of men under 30 now describe themselves as single — compared with 34% of women the same age[2]. Fifteen percent of men report having zero close friends, up fivefold from 3% in 1990[3]. In the UK, suicide is the single leading cause of death for men under 50[4].
You're going to hear that these are separate problems. They aren't. This article makes the case — with peer-reviewed data — that the testosterone decline and the male loneliness epidemic are part of the same story. It also covers something Napoleon Hill understood in 1937 that most men today have completely forgotten: what happens to male drive when it goes unfed, and what the most driven men in history did with it instead.
The Decline Is Real, Documented, and Getting Worse
The landmark study remains Travison et al. (2007), published in the Journal of Clinical Endocrinology & Metabolism. Using data from 1,532 men across three waves of the Massachusetts Male Aging Study (1987–2004), they found an age-independent population-level decline of 1.2% per year — median testosterone falling from 501 ng/dL to 391 ng/dL, regardless of BMI, smoking, or lifestyle[5].
Lokeshwar et al. (2021) analysed NHANES data from 4,045 men aged 15–39 and found mean total testosterone had fallen from 605 ng/dL to 451 ng/dL in under two decades. Even normal-weight young men showed a 20% decline. Obesity alone does not explain this[1].
In 2025, Santi et al. published a systematic review in the Journal of Endocrinological Investigation pooling 1,256 papers covering over one million men from 1971 to 2024. Annual decline: 0.56% per year. Critically, LH — the brain signal that tells the testes to produce testosterone — is declining too. The problem begins in the hypothalamus itself[6].
📉 The Testosterone Decline — What the Research Shows Across Generations
1987Baseline
Massachusetts Male Aging Study — Wave 1
Median total testosterone in American men: 501 ng/dL. This becomes the reference point against which all subsequent data is measured.[5]
200417 Yrs Later
Massachusetts Male Aging Study — Wave 3
Median total testosterone: 391 ng/dL. A 22% decline — independent of age, BMI, and lifestyle. A 60-year-old in 2004 had significantly lower T than a 60-year-old in 1987.[5]
2000–16Young Men
NHANES — Men Aged 15–39
Mean testosterone falls from 605 to 451 ng/dL — a 25% collapse in under two decades. Even normal-weight young men show a 20% decline. Obesity alone is not the cause.[1]
1942–51vs Earlier
Finnish Cohort Study — Generational Comparison
Men born 1942–1951 had testosterone of 13.8 nmol/L vs 21.9 nmol/L in those born 1913–1922 at the same age — a 37% generational drop.[7]
2025Latest Data
Santi et al. — 1M+ Men, 53 Years of Data
Meta-regression of 1,256 papers, 1,064,891 men, 1971–2024. Confirmed annual decline of ~0.56% per year. LH levels also declining — the HPG axis itself is being suppressed.[6]
Sources: Travison et al., JCEM 2007[5]; Lokeshwar et al., European Urology Focus 2021[1]; Perheentupa et al., Eur J Endocrinol 2013[7]; Santi et al., J Endocrinol Invest 2025[6]
Testosterone Doesn't Just Build Muscle. It Builds Men.
The cultural conversation around testosterone obsesses over gym performance and libido. That misses the bigger story. Testosterone is the neurochemical substrate of male confidence, social approach, and competitive drive.
🧠
Fear & Approach
Biases the amygdala toward threat approach, not avoidance — rewires the brain to move toward challenges
👊
Dominance
Drives assertiveness, social influence, and status-seeking behaviour — not just aggression
📈
Risk Tolerance
Morning T predicts day's trading profitability; linked to entrepreneurial intent and career ambition
🤝
Mate Attraction
T-linked facial masculinity predicts women's mate attractiveness ratings in peer-reviewed studies
💬
Social Confidence
Higher endogenous T predicts symptom reduction in social anxiety — and reduces gaze avoidance
🔥
Drive & Vigour
Low T clinical profile: lack of assertiveness, low vigour, dysphoria, depression — published in Andrology 2020
1. Confidence and Social Approach
Multiple studies show testosterone directly modifies the brain's threat-response system. Radke et al. (2015) demonstrated in Science Advances that testosterone biases the amygdala toward threat approach rather than avoidance — it literally rewires the system responsible for processing social threat to move toward challenges rather than away from them[8].
Enter et al. (2016) showed testosterone administration reduced gaze avoidance in social anxiety disorder — a disorder characterised by active avoidance of eye contact and social situations. Subsequent research confirmed that endogenous testosterone levels predict how well men respond to exposure therapy for social anxiety[9].
Saj — Founder, SALIENTS®
The gaze avoidance finding hit close to home for me. When I was single, I remember actively avoiding eye contact with women I found attractive — not consciously, not deliberately, just a kind of automatic flinching away. I thought it was just shyness. I didn't have a framework for it.
I notice now that I don't do that anymore. I can hold a glance, acknowledge someone, move on without it being a whole internal event. It's a small thing. But small things compound. That's the gap the research is describing — not some dramatic personality transformation, just the difference between a brain wired to approach and one wired to retreat. Thousands of small moments, across years, that add up to very different lives.
Higher testosterone doesn't just correlate with confidence — it causes it. At a neurological level, it changes how the brain processes social threat.
The mechanism is not subtle. Low testosterone produces a recognisable clinical profile: lack of assertiveness, low vigour, dysphoria, reduced drive. Zitzmann (2020) in Andrology documented this comprehensively, noting that individual differences in androgen receptor sensitivity modulate how strongly these effects manifest — meaning some men experience the consequences of even modest testosterone decline more acutely than others[10].
2. Risk Tolerance and Ambition
The link between testosterone and economic and entrepreneurial behaviour is now well-documented. Coates & Herbert (2008) in PNAS tracked 17 London traders over eight days and found morning testosterone predicted that day's profitability — on a six-day winning streak, one trader's testosterone rose 74%[11].
Sapienza, Zingales & Maestripieri (2009), also in PNAS, studied over 500 MBA students and found testosterone predicted both risk tolerance and career self-selection into high-risk, high-reward industries[12]. White et al. (2006) found testosterone was positively associated with risk propensity in MBA students and that this translated into real entrepreneurial experience[13].
💡
Falling testosterone doesn't just produce quieter men. It produces less ambitious ones. The research doesn't just show a correlation between T and ambition — it shows testosterone actively drives the instinct to take calculated risks, compete for status, and back yourself.
3. The Biology of Being Single
Research consistently finds that single men have higher testosterone than partnered men[14][15]. This is partly causal — testosterone drives the competitive, approach-oriented behaviour that leads to mate acquisition in the first place.
Roney et al. (2006) in Proceedings of the Royal Society B demonstrated that men's testosterone concentrations predicted women's ratings of their facial masculinity, and that testosterone-linked features specifically predicted short-term attractiveness[16]. Voice pitch — a testosterone-dependent trait — is consistently rated as more masculine and attractive.
📊 The Cascade — How Low T Reduces Relationship Likelihood
Low TRoot cause
The trigger
Less ApproachSocial anxiety
Amygdala avoidance bias ↑
Less DriveRisk aversion
Ambition & status-seeking ↓
Less AttractiveMate selection
Masculine cues reduced → fewer opportunities
Synthesised from: Radke et al., Science Advances 2015[8]; Enter et al., Clin Psychol Sci 2016[9]; Roney et al., Proc Royal Soc B 2006[16]; Mazur & Booth, Behav Brain Sci 1998[17]
The chain is biologically coherent: lower testosterone → reduced social approach → less assertive self-presentation → fewer visible masculine cues → reduced partner acquisition. This is not sociology. It is endocrinology.
4. The Wider Collapse
Testosterone decline is one signal in a much larger pattern of male biological and social deterioration.
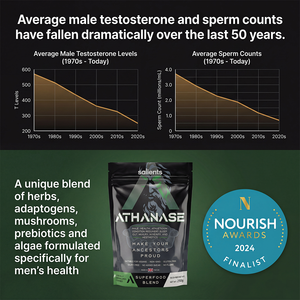
Sperm counts have halved. Levine et al. (2017) in Human Reproduction Update — a meta-analysis of 185 studies covering 42,935 men — found sperm concentration in Western men declined 52.4% between 1973 and 2011. Their 2023 update found the global decline is accelerating, now at 2.48% per year worldwide[18].
Male obesity has tripled. Global male obesity rose from 4.8% in 1990 to 14.0% in 2022 (The Lancet, 2024). In the US, 39.2% of men are now obese. Over 72% are overweight or obese[19]. Adipose tissue contains aromatase — the enzyme that converts testosterone to oestrogen. Obesity suppresses T and the suppressed T accelerates obesity. It is a self-reinforcing loop.
Men are dying by their own hand at epidemic rates. In the US, men account for approximately 80% of all suicides — roughly 39,000 deaths per year, at a rate four times that of women. In the UK, suicide is the single leading cause of death for men under 50[4]. 40% of British men have never spoken to anyone about their mental health[20].
15% of men now report having zero close friends — up from 3% in 1990. These are not cultural quirks. They are the downstream consequences of a hormonal and behavioural deterioration playing out at population scale. — Survey Center on American Life, 2021[3]
5. What Is Causing the Collapse
The decline has no single cause. It is the convergence of multiple modern inputs simultaneously suppressing male hormonal function.
Processed Food
A 75g glucose load caused a 25% acute testosterone drop in 74 men — 15% fell into hypogonadal range within two hours. Ultra-processed foods now make up ~55% of Western daily calories.[21]
Sleep Loss
One week of five-hour nights reduces daytime testosterone 10–15% in young men — the equivalent of ageing 10–15 years. Most testosterone is produced during sleep.[22]
Endocrine Disruptors
Phthalate metabolites linked to 24–34% testosterone reductions in boys aged 6–12. BPA exposure correlated with dramatically increased male sexual dysfunction risk. These chemicals are in plastic packaging, receipts, and personal care products.[23]
Chronic Stress
Sustained high cortisol directly inhibits GnRH release, suppressing LH, FSH, and testicular testosterone production. Cortisol and testosterone are physiological antagonists.[24]
Sedentary Life
A UK Biobank analysis of 208,677 men found physically inactive men had testosterone ~58 ng/dL lower than active counterparts — independent of BMI.[25]
Alcohol
A 2024 meta-analysis of 21 studies confirmed chronic alcohol reduces total testosterone by ~4 nmol/L while elevating estradiol. The gonadal axis is directly suppressed.[26]
6. What the Evidence Says About Fighting Back
The same research that documents the crisis also points clearly toward interventions that work — without pharmaceutical intervention.
Resistance training with compound movements (squats, deadlifts, presses) at high intensity produces significant acute testosterone elevations and, through sustained body composition improvements, supports long-term hormonal health. A UK Biobank analysis confirmed this at population scale. The training must be heavy and effortful — nothing else produces the same response.
Sleep of 7–9 hours is not a luxury — it is a hormonal requirement. The majority of daily testosterone is produced during sleep. Leproult & Van Cauter (2011) showed just one week of restricted sleep has measurable hormonal consequences[22].
Micronutrient sufficiency matters. Zinc deficiency nearly halves testosterone — correction nearly doubles it (Prasad et al., 1996). Magnesium at 450mg/day raised testosterone 24% in four weeks (Cinar et al., 2011). Vitamin D supplementation at 3,332 IU/day raised testosterone 25% in deficient men (Pilz et al., 2011)[27].
📊 Evidence-Based Botanicals — Key Trials
Data from: Wankhede et al., JISSN 2015 (KSM-66®)[28]; Rao et al., Aging Male 2016 (Fenugreek)[29]; Pandit et al., Andrologia 2016 (Shilajit)[30]. All RCTs, placebo-controlled. Values show % increase in total testosterone vs baseline over trial duration.
Several botanical compounds carry meaningful clinical evidence. KSM-66® Ashwagandha produced a testosterone increase of 96.2 ng/dL versus 18.0 ng/dL in placebo over 8 weeks in resistance-training men[28]. Shilajit produced a 20.45% increase in total testosterone and 31.35% increase in DHEA-S in a 90-day double-blind RCT[30]. Fenugreek has been shown in multiple RCTs to reduce testosterone conversion to oestrogen and DHT, supporting free testosterone levels[29].
7. The Drive Problem Nobody Talks About
Here is something the wellness industry won't say out loud: sexual frustration, properly channelled, is one of the most powerful motivational forces a man possesses.
Napoleon Hill wrote about it in 1937. Sigmund Freud theorised it. Every serious tradition of male self-mastery has acknowledged it in some form. The desire for connection — physical, sexual, relational — does not disappear when it goes unmet. It either turns inward and festers, producing the anxious, passive, scrolling man so common today, or it gets transmuted into productive energy: training harder, building more, competing more fiercely.
The difference between those two outcomes is not willpower. It is vitality. A man whose libido is suppressed — by low testosterone, chronic stress, poor sleep, or processed food — does not have a drive problem he can simply think his way out of. The engine is running low. There is less raw energy to redirect in the first place.
The desire for connection doesn't disappear when it goes unmet. It either festers — or it becomes fuel. The difference is whether you have the vitality to transmute it.
This is where the evidence on Maca Root becomes particularly relevant. Unlike ashwagandha or shilajit, maca does not raise serum testosterone — this is clearly established by peer-reviewed research[31]. Its effects operate through entirely different pathways. Gonzales et al. (2002) in a double-blind, placebo-controlled trial found that maca significantly improved self-reported sexual desire from week 8 onward, independent of testosterone levels or mood changes[32]. The active compounds — macamides and glucosinolates — appear to act on the central nervous system and hypothalamus rather than the gonads.
What this means practically: maca supports the subjective experience of drive and desire. Not as a pharmaceutical intervention. As a nutritional input that supports what the male body is designed to produce when properly nourished. Used by Andean warriors and labourers for over 2,000 years — at altitude, under physical stress, with physically demanding lives — it was not regarded as a supplement. It was regarded as food.
🔥
The argument is simple: a man with healthy libido and redirected drive is not a man sitting idle on a Saturday afternoon. He is training, building, competing, creating. Sexual vitality and productive ambition are not in tension with each other — they draw from the same biological reservoir. Deplete one and you deplete both.
8. Athletic Performance — The Other Half of the Equation
The hormonal story and the performance story are not separate narratives. They are the same one.
KSM-66® Ashwagandha — beyond its hormonal effects — has one of the most robust athletic performance evidence bases of any botanical compound. Wankhede et al. (2015) found that men taking 600mg/day for 8 weeks gained significantly more muscle mass, lost more body fat, and recovered faster than the placebo group — with the testosterone data simply confirming the mechanism[28]. A separate study confirmed significant improvements in VO2 max and cardiorespiratory endurance in elite cyclists[33].
Guarana — present in ATHANASE® at 500mg — provides a sustained release of naturally occurring caffeine, with additional xanthines and antioxidants that modulate its release differently to coffee. A review published in Nutrients confirmed guarana's cognitive and physical performance benefits, with the sustained-release profile producing fewer of the crash and anxiety effects associated with high-dose caffeine[34].
Ginger, at 250mg per serving, has a meaningful anti-inflammatory evidence base relevant to training recovery. A meta-analysis of 16 RCTs confirmed significant reductions in exercise-induced muscle soreness — both delayed onset (DOMS) and immediate post-exercise pain — with daily ginger supplementation[35]. In the context of consistent training, reduced soreness means more sessions, better quality work, and compounding results over time.
Siberian Ginseng (Eleuthero) has been studied in athletic contexts since Soviet-era sports science in the 1960s. More recent research published in the Journal of the International Society of Sports Nutrition confirmed that 8 weeks of supplementation significantly improved endurance capacity, with athletes running further and faster than placebo by week 8[36].
💪
Muscle & Recovery
KSM-66® Ashwagandha — significantly greater muscle gain, fat loss, and recovery vs placebo in 8-week RCT
⚡
Sustained Energy
Guarana 500mg — naturally occurring caffeine with extended release profile, supporting focus and physical output without hard crash
🔄
Inflammation & Soreness
Ginger 250mg — meta-analysis of 16 RCTs confirms significant reduction in exercise-induced muscle soreness
🏃
Endurance
Siberian Ginseng — 8 weeks significantly improved endurance capacity vs placebo in trained athletes
🔥
Drive & Desire
Maca Root 1,750mg — the largest dose in the formula. Peer-reviewed evidence for improved sexual desire from week 8, independent of testosterone
⚖️
Hormone Balance
Fenugreek + Shilajit + KSM-66® working across three separate mechanisms to support the body's own hormonal environment

ATHANASE® — Three Pillars. One Formula.
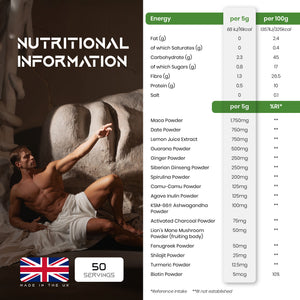
Hormonal support. Athletic performance. Drive and vitality. ATHANASE® is built across all three — 16 whole-food ingredients, each selected on peer-reviewed evidence. KSM-66® Ashwagandha, Maca Root, Shilajit, Fenugreek, Guarana, Siberian Ginseng, Ginger, and nine more. No fillers. No artificial flavourings or colourings. Informed Sport certified. One 5g daily serving.
View the Full Formula →What Your Ancestors Had That You Don't
Your great-great-grandfather didn't optimise his morning routine. He didn't track his macros or read about testosterone on the internet. But he almost certainly had more of it than you do — and the reason is not genetic. It's environmental.
He moved heavy things daily. He slept when it got dark. He ate real food without packaging. He faced genuine physical and social risk regularly — the kind of challenges that spike testosterone rather than suppress it. He had a community, a role, a clear sense of what was expected of him. His cortisol was acute and short-lived, not chronic and grinding. His food didn't come wrapped in endocrine-disrupting plastics. His body was not marinated in synthetic compounds from birth.
None of this is nostalgia. It's biology. The inputs that produce healthy testosterone in men are the same inputs they have always been. The modern world has systematically removed them — and replaced them with processed food, artificial light, sedentary work, and chemical exposure at every turn. The result is the data you've read above.
The path back is not complicated. It is just countercultural. Train hard. Sleep enough. Eat real food. Manage your stress. Know what you're putting into your body. These are not biohacks. They are the conditions your endocrine system was built to operate within.
The Bottom Line
Across five decades and over a million men, testosterone is declining at roughly 0.5–1.0% per year. It cannot be attributed to ageing. It cannot be explained by obesity alone. It is happening to young men in their twenties, healthy-weight men who have done nothing to deserve it except live inside the modern world.
The downstream consequences — collapsing sperm counts, epidemic loneliness, male suicide as a leading cause of death — are not isolated cultural phenomena. They are the predictable outcome of a hormonal and behavioural deterioration playing out at population scale.
And the drive problem Napoleon Hill wrote about in 1937 is the same one playing out now — except the men of his era had the vitality to transmute it into something. The question is whether today's men have the same raw material to work with. That starts with what you put in your body, how you train, and how seriously you take your own biology.
Make Your Ancestors Proud®
The energy has to come from somewhere. ATHANASE® is the nutritional foundation — built for men who understand that vitality is not a luxury, it's the engine everything else runs on.
KSM-66® Ashwagandha · Maca Root 1,750mg · Shilajit · Fenugreek · Guarana · Siberian Ginseng · Ginger · and 9 more
Informed Sport Certified · No artificial flavourings, colourings, emulsifiers or fillers · Used by boxers, lifters, and men who give a damn
Shop ATHANASE®Make Your Ancestors Proud! ⚔️
📚 References
[1] Lokeshwar, S.R. et al. (2021). Decline in Serum Testosterone Levels Among Adolescent and Young Adult Men in the USA. European Urology Focus, 7(4), 886–889. PubMed
[2] Pew Research Center (2023). 5 Facts About Single Americans. pewresearch.org
[3] Survey Center on American Life (2021). Men's Social Circles Are Shrinking. American Enterprise Institute. americansurveycenter.org
[4] London Assembly (2024). Suicide — the single leading cause of death for men under 50. Greater London Authority.
[5] Travison, T.G. et al. (2007). A Population-Level Decline in Serum Testosterone Levels in American Men. JCEM, 92(1), 196–202. PubMed
[6] Santi, D. et al. (2025). Temporal Trends in Serum Testosterone and LH Levels: A Systematic Review. Journal of Endocrinological Investigation. Springer
[7] Perheentupa, A. et al. (2013). A cohort effect in serum testosterone levels in Finnish men. European Journal of Endocrinology, 168(2), 227–233.
[8] Radke, S. et al. (2015). Testosterone biases the amygdala toward social threat approach. Science Advances, 1(6). ScienceDaily
[9] Enter, D., Spinhoven, P. & Roelofs, K. (2016). Dare to Approach. Clinical Psychological Science, 4(2), 200–210. See also: Psychoneuroendocrinology, 115, 2020.
[10] Zitzmann, M. (2020). Testosterone, mood, behaviour and quality of life. Andrology, 8(6), 1598–1605. Wiley
[11] Coates, J.M. & Herbert, J. (2008). Endogenous steroids and financial risk taking on a London trading floor. PNAS, 105(16), 6167–6172. PNAS
[12] Sapienza, P., Zingales, L. & Maestripieri, D. (2009). Gender differences in financial risk aversion and career choices are affected by testosterone. PNAS, 106(36), 15268–15273.
[13] White, R.E., Thornhill, S. & Hampson, E. (2006). Entrepreneurs and evolutionary biology: testosterone and new venture creation. Organizational Behavior and Human Decision Processes, 100(1), 21–34.
[14] Burnham, T.C. et al. (2003). Men in committed, romantic relationships have lower testosterone. Hormones and Behavior, 44(2), 119–122.
[15] Booth, A. & Dabbs, J.M. (1993). Testosterone and men's marriages. Social Forces, 72(2), 463–477.
[16] Roney, J.R. et al. (2006). Reading men's faces: women's mate attractiveness judgments track men's testosterone. Proc Royal Society B, 273(1598), 2169–2175.
[17] Mazur, A. & Booth, A. (1998). Testosterone and dominance in men. Behavioral and Brain Sciences, 21(3), 353–397.
[18] Levine, H. et al. (2022). Temporal trends in sperm count: a systematic review and meta-regression. Human Reproduction Update. PubMed
[19] NCD Risk Factor Collaboration (2024). Worldwide trends in underweight and obesity. The Lancet.
[20] Priory Group (2019). Men's Mental Health Survey. priorygroup.com
[21] Caronia, L.M. et al. (2013). Abrupt decrease in serum testosterone after an oral glucose load. Clinical Endocrinology, 78(2), 291–296. PubMed
[22] Leproult, R. & Van Cauter, E. (2011). Effect of 1 week of sleep restriction on testosterone in young healthy men. JAMA, 305(21), 2173–2174.
[23] Meeker, J.D. & Ferguson, K.K. (2014). Urinary phthalate metabolites are associated with decreased serum testosterone. JCEM, 99(11), 4346–4352.
[24] Mehta, P.H. & Josephs, R.A. (2010). Testosterone and cortisol jointly regulate dominance: evidence for a dual-hormone hypothesis. Hormones and Behavior, 58(5), 898–906.
[25] UK Biobank analysis cited in: Understanding the Secular Decline in Testosterone, MDPI International Journal of Molecular Sciences, 2025.
[26] Santi, D. et al. (2024). Chronic alcohol consumption influences the gonadal axis in men: meta-analysis. Andrology, 13(2). Wiley
[27] Pilz, S. et al. (2011). Effect of vitamin D supplementation on testosterone levels in men. Hormone and Metabolic Research, 43(3), 223–225.
[28] Wankhede, S. et al. (2015). Examining the effect of Withania somnifera supplementation on muscle strength and recovery. JISSN, 12(43). Nutritional Outlook
[29] Rao, A. et al. (2016). Testofen reduces age-related symptoms and increases testosterone levels in healthy aging males. Aging Male, 19(2), 134–142. PubMed
[30] Pandit, S. et al. (2016). Clinical evaluation of purified Shilajit on testosterone levels in healthy volunteers. Andrologia, 48(5), 570–575. Wiley
[31] Gonzales, G.F. et al. (2003). Effect of Lepidium meyenii (Maca) on sexual desire and its absent relationship with serum testosterone levels in adult healthy men. Andrologia, 35(6), 367–372. PubMed
[32] Gonzales, G.F. et al. (2002). Effect of Lepidium meyenii (MACA) on sexual desire and its absent relationship with serum testosterone levels. Andrologia, 34(6), 367–372. PubMed
[33] Shenoy, S. et al. (2012). Effects of eight-week supplementation of Ashwagandha on cardiorespiratory endurance in elite Indian cyclists. Journal of Ayurveda and Integrative Medicine, 3(4), 209–214.
[34] Moustakas, D. et al. (2015). Guarana provides additional stimulation over caffeine alone. PLOS ONE, 10(4). See also systematic review in Nutrients 2021 on guarana's cognitive and physical effects.
[35] Hoseinzadeh, K. et al. (2015). Acute effects of ginger extract on delayed onset muscle soreness. Medical Journal of the Islamic Republic of Iran. See also: Black, C.D. et al., Phytotherapy Research 2010 — meta-analysis of ginger and exercise-induced muscle soreness.
[36] Kuo, J. et al. (2010). The effect of eight weeks of supplementation with Eleutherococcus senticosus on endurance capacity and metabolism. JISSN, 7(33).
⚠️ Important Information
This article is for educational purposes only and does not constitute medical advice. ATHANASE® is a food supplement and is not intended to diagnose, treat, cure, or prevent any disease. If you have a pre-existing medical condition or concerns about your hormone levels, please consult a qualified healthcare professional.
The World's First Superfood Blend For Men
































£28.00
MAKE YOUR ANCESTORS PROUD® with ATHANASE®. A blend of herbs, adaptogens, mushrooms, prebiotic and algae. Specially formulated for men, to help conquer 7 areas:
| |
MALE HEALTH |
| |
ATHLETICISM |
| |
MOOD & COGNITION |
| |
RECOVERY & SLEEP |
| |
GUT HEALTH |
| |
IMMUNITY |
| |
AESTHETICS |
Select a purchase option to pre order this product
Countdown header